Why were four times more girls than boys referred to the Tavistock last year from Ireland?
A 2014 survey of adults attending a Dublin gender clinic found suspected or confirmed gender dysphoria in nearly three times as many men as women. But last year four times as many girls as boys were referred from here to the UK's Gender Identity Development Services. Why is this?

In 2014 Prof Donal O'Shea and colleagues at St Columcille's Hospital in Loughlinstown retrospectively surveyed those with suspected or confirmed gender dysphoria between 2005 and early 2014.
"The prevalence of GD in the Irish population was 1:10,154 male-to-female (MTF) and 1:27,668 female-to-male (FTM), similar to reported figures in Western Europe."
Almost 73% (159) were men, with only 59 being women. The average age was 32 for both sexes. So in adults it was a nearly 3:1 ratio of males to females.
Children under 18 are referred from Ireland to the Gender Identity Development Service (GIDS) at the UK's Tavistock and Portman NHS Foundation Trust
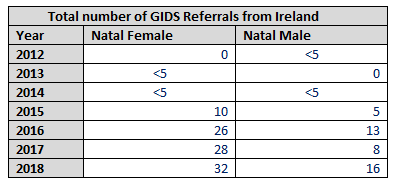


The Tavistock clarified that the "The difference can be accounted for due to the difference in number between “referred” and “seen” young people from Ireland."
From 2015 onwards the numbers grew from 15 to 48 in 2018 when there were twice as many girls referred from here as boys. In March this year the Tavistock said that

So last year the numbers of girls referred from Ireland rose to four times that of boys. This mirrors a trend seen elsewhere of more teenage girls exhibiting gender distress.
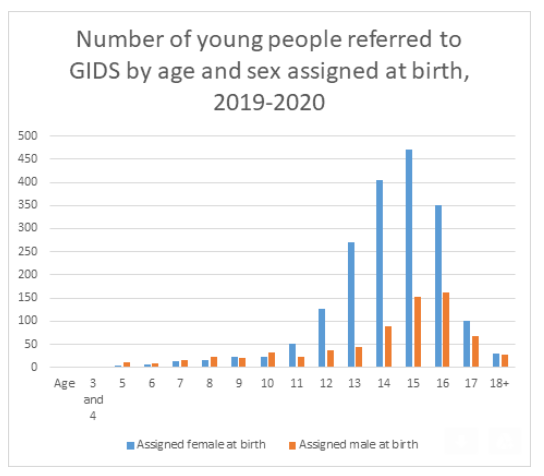
(Note: sex is not "assigned" at birth, it's observed)
Why are more girls in Ireland distressed about their gender identity?
In January 2020 an international study carried out across 47 countries and regions in conjunction with the World Health Organisation found that when compared with the other 46 countries that participated, Irish children "fare very well in reporting happiness in their lives".
However the researcher Aoife Gavin said that "But I think in particular we should be focusing on the girls, and the older girls - the 15 to 17 year old girls. They're significantly more likely to report being unhappy or poor life satisfaction." Is there any risk that this might have an impact on the numbers feeling distress over their gender?
What do medical experts in the area have to say?
In their submission to the Gender Recognition Act Review Group (2018) St. Patrick's Mental Health Services - which caters not only for adults but also for adolescents of 12 - 18 years - said that
“Dutch research has examined developmental trajectories of persistence and desistence of childhood gender dysphoria/distress. The Center of Expertise on Gender Dysphoria at the VU University Medical Center Amsterdam has one of the longest-established specialist gender clinics in the world. Their reports revealed that most children (approx. 80%) with gender dysphoria will not remain gender dysphoric after puberty. Therefore, caution must be used with changes in pre-pubertal youth.
It is important that all possibilities are kept open for the future. Young people increasingly present with possession of gender variant feelings for a relatively short period of time. They have a right and need to be given sufficient time to process these feelings. If they do not have sufficient time to process these feelings, which may change over time they may later regret a legal transition.
Gender variance does not constitute a mental health illness. However, there are well documented high rates of co-occurring mental health difficulties, self-harming behaviour, suicidal ideation and high rates of comorbid Autistic Spectrum Disorders.”
Professor Donal O'Shea, Consultant Endocrinologist, as part of a submission made by the Royal College of Physicians of Ireland submitted to the Review Group that
"In recent years there has been a change in pattern of referral of patients to our service with a younger age profile and a significant increase in individuals with gender confusion, gender fluidity and Autistic Spectrum behaviour. This does not impact on the gender issue for the individual but may impact on suitability to progress. Medical and surgical treatment of an individual with gender confusion or fluidity will be regretted."
and
"An issue with gender is not the same as gender Dysphoria requiring gender reassignment. In our service where over 300 patients have attended we have had 3 individuals who have regretted their gender reassignment post operatively and several who have stopped their transitioning journey at various points. That is not to say they did not have gender issues, rather it was that hormonal and surgical reassignment was not appropriate in their overall situation. This can be as a result of autistic spectrum issues, personality issues or developmental disorders."
Meanwhile the Irish College of General Practitioners pointed out that
“Currently GP’s are not trained in the medical aspects of gender recognition or in the area of counselling individuals regarding the medical, legal and constitutional consequences of gender reassignment and gender recognition. Therefore the GP has no formal role to play in decision making in this act, other than to possibly be the doctor involved in making the initial referral to specialists in the field, and to coordinating the updating of patients medical records with new information from specialists who were involved in caring for the patient.“
No one is born with a gender. Everyone is born with a biological sex. Gender (an awareness and sense of oneself as male or female) is a sociological and psychological concept; not an objective biological one. No one is born with an awareness of themselves as male or female; this awareness develops over time and, like all developmental processes, may be derailed by a child’s subjective perceptions, relationships, and adverse experiences from infancy forward. People who identify as “feeling like the opposite sex” or “somewhere in between” do not comprise a third sex. They remain biological men or biological women.
A person’s belief that he or she is something they are not is, at best, a sign of confused thinking. When an otherwise healthy biological boy believes he is a girl, or an otherwise healthy biological girl believes she is a boy, an objective psychological problem exists that lies in the mind not the body, and it should be treated as such. These children suffer from gender dysphoria. Gender dysphoria (GD), formerly listed as Gender Identity Disorder (GID), is a recognized mental disorder in the most recent edition of the Diagnostic and Statistical Manual of the American Psychiatric Association (DSM-5). The psychodynamic and social learning theories of GD/GID have never been disproved.
Puberty is not a disease and puberty-blocking hormones can be dangerous. Reversible or not, puberty-blocking hormones induce a state of disease –the absence of puberty –and inhibit growth and fertility in a previously biologically healthy child.
According to the DSM-5, as many as 98% of gender confused boys and 88% of gender confused girls eventually accept their biological sex after naturally passing through puberty.
Pre-pubertal children diagnosed with gender dysphoria may be given puberty blockers as young as eleven, and will require cross-sex hormones in later adolescence to continue impersonating the opposite sex. These children will never be able to conceive any genetically related children even via artificial reproductive technology. In addition, cross-sex hormones (testosterone and oestrogen) are associated with dangerous health risks including but not limited to cardiac disease, high blood pressure, blood clots, stroke, diabetes, and cancer.
Rates of suicide are nearly twenty times greater among adults who use cross-sex hormones and undergo sex reassignment surgery, even in Sweden which is among the most LGBTQ –affirming countries. What compassionate and reasonable person would condemn young children to this fate knowing that after puberty as many as 88%of girls and 98% of boys will eventually accept reality and achieve a state of mental and physical health?
The Gender Recognition Act Review Group reported that “Some of the Review Group members raised queries about a link with autism. In this regard, an extended diagnostic period is preferred by doctors as in their opinion some children presenting with autism, while highly functioning, are vulnerable and can have very fixed views, and need to be fully protected and supported. It was also felt that there are benefits to be gained from taking time with them to think through the implications of their decision.”.
Despite the experts concerns the Gender Recognition Act Review Group recommended self-id for children “of any age”, along with legal gender recognition for the “non-binary” in July 2018.
In November 2019 Minister Regina Doherty agreed to legal gender self-id recognition for children aged 16/17 years. The minister said
"The measures I am proposing today aim to reform this process to reflect the fact that the legal recognition of a person’s gender is separate and distinct from any question of medical intervention, and should be facilitated with parental consent and a simple revocation process.”